
Childhood growth is a mirror for “the material and moral condition” of a society.
– Dr. James Tanner, pediatrician and auxologist (1986:3)
.
In 2015, Lital Keinan-Boker and colleagues published a study in The Israel Medical Association Journal that examined whether the Holocaust during WW2 had impacted the long-term health of older Israeli adults (mean age 69 years). They were working within the framework of the Developmental Origins of Health and Disease (DOHaD) paradigm, a body of evidence that shows that an array of stressors including malnutrition early in life (prenatally and/or during infancy) can increase risk for various chronic diseases in adulthood.
The study design compared people who were born between 1940–1945 in Nazi-occupied countries in Europe (which they categorized as the ‘exposed’ group; n=653) to those in Israel to Europe-born parents (‘non-exposed’; n=433). After adjusting for confounding variables, Keinan-Boker et al concluded that those born in Europe during WW2 were significantly more likely to have dyslipidemia, type 2 diabetes, hypertension, and cardiovascular disease. As they wrote, “The results of the current study on fetal and early childhood exposure to malnutrition and hunger and the subsequent long-term outcomes are in accordance with previously published data from research on non-Jewish populations.”
Indeed. There is nothing unique about this study or population. Quite the opposite. Epidemiological evidence is now fairly robust that armed conflicts and (often anthropogenic) famines can leave a deleterious lasting mark on very young bodies, which can endure for decades. While the specific health outcomes vary by study, the pattern holds true whether we are talking about Israelis born in Europe during the Holocaust, the Dutch Hunger Winter (Painter et al. 2005), the siege of Leningrad (Stanner et al. 1997; Koupil et al. 2007), the Spanish Civil War (González Zapata et al. 2006), the Biafran famine during the Nigerian Civil War (Hult et al. 2010), the Holodomor in Ukraine (Lumey et al 2015), France during WW2 (Allais et al. 2021), or the First and Second Indochina Wars in Laos (Clarkin 2008). This is not an Israeli thing. It is a human thing, likely even a mammalian thing. It is how young bodies often respond to the harsh stresses and deprivation and war, at least for those who survive.
Which brings us to Gaza.

.
Two weeks ago, UNICEF reported that the prevalence of acute malnutrition among infants 0 to 2 years old in northern Gaza had risen to 31%, double the rate it had been in January (15.6%). This was the nearly inevitable result of the massive destruction there (as one reporter put it, Gaza City is “more rubble now than city”), as well as Israeli forces blocking food aid into Gaza, and —air drops aside— a lack of other adequate humanitarian assistance such as therapeutic foods. Screenings revealed that other parts of Gaza also have high rates of acute malnutrition, including Khan Younis (28%), and Rafah (10%) in the south.
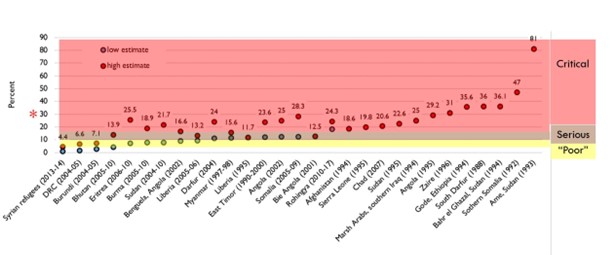
Humanitarian organizations use the rate of acute malnutrition (ascertained by a weight-for-height or arm circumference well below average) as a gauge of population health. The WHO uses the following community thresholds for acute malnutrition in 0–5 year-olds (WHO 2000: 40):
<5% = acceptable
5% to 9.9% = poor
10% to 14.9% = serious
15% + = critical
The rates given by UNICEF applied to 0-2 year olds in Gaza, rather than 0-5, but the WHO cutoffs give us a sense of how dire the situation is. For further context, below are rates of acute malnutrition from various conflicts and displaced people I collated from various sources, colored by WHO cutoff thresholds. The red asterisk on the left is the rate for North Gaza two weeks ago. The 31% figure would fall along the high end of some of the worst humanitarian disasters in recent history. This is consistent with Oxfam’s recent estimation that the daily death rate in Gaza has been much higher than other recent conflicts, including Syria, Sudan, Ukraine, Afghanistan, and Yemen.
.
Of course, it’s not just infants who are suffering. There have been an estimated 20,000 births in Gaza since the Oct 7 Hamas attack, reminding us of the stressors faced during pregnancy. A report from NPR summarized the situation like this:
.
Amid a spiraling humanitarian crisis, women who are pregnant or have recently given birth are confronting impossible conditions as they grapple with how to care for their newborns. In place of celebrations and nursery rhymes, they face airstrikes and ground fighting. Instead of bottles and baby food, they’re fighting disease and a growing lack of food and water.
“I can’t teach her to eat or feed her because there’s no food, no vegetables, and there’s not enough milk for her,” (new mother Likka) Saleh says. “I can’t sleep at night because all I’m doing is thinking and I’m heartbroken.”
.
Like the Holocaust, the Dutch Hunger Winter, Leningrad, France, Biafra, Laos, and the Holodomor we can expect this manmade disaster to linger in the bodies of children just born, and yet to be born, in Gaza.
When adding up the costs of armed conflict —the deaths, amputations, psychological trauma, lost family, razed neighborhoods, the hunger and tears, the feeling of being abandoned, the wounded souls, the lost education, the time wasted and dreams dashed, the broken trust, the resentment at being pushed toward hatred— somewhere in the ledger we need to acknowledge the long-term costs to health. It is another added tax, in this case to be paid by the youngest people who’ve just arrived on this planet, who have harmed no one.
.
References
Allais O, Fagherazzi G, Mink J. 2021 The long-run effects of war on health: Evidence from World War II in France. Social Science & Medicine. 276:113812.
Clarkin PF. 2008. Adiposity and height of adult Hmong refugees: relationship with war-related early malnutrition and later migration. Am. J. Hum. Biol. 20(2):174–84
González Zapata LI, Alvarez-Dardet Díaz C, Nolasco Bonmatí A, Pina Romero JA, Medrano MJ. 2006. Famine in the Spanish civil war and mortality from coronary heart disease: a perspective from Barker’s hypothesis. Gac. Sanit. 20(5):360–67
Hult M, Tornhammar P, Ueda P, Chima C, Bonamy A-KE, et al. 2010. Hypertension, diabetes and overweight: looming legacies of the Biafran famine. PLoS One. 5(10):e13582
Keinan-Boker L, Shasha-Lavsky H, Eilat-Zanani S, Edri-Shur AE, Shasha SM. 2015. Chronic health conditions in Jewish Holocaust survivors born during World War II. The Israel Medical Association Journal 17(4):206–12.
Koupil I, Shestov DB, Sparén P, Plavinskaja S, Parfenova N, Vågerö D. 2007. Blood pressure, hypertension and mortality from circulatory disease in men and women who survived the siege of Leningrad. Eur. J. Epidemiol. 22(4):223–34
Lumey LH, Khalangot MD, Vaiserman AM. 2015. Association between type 2 diabetes and prenatal exposure to the Ukraine famine of 1932–33: a retrospective cohort study. Lancet Diabetes Endocrinol. 3(10):787–94
Lutfy C, Cookson ST, Talley L, Rochat R. 2014. Malnourished children in refugee camps and lack of connection with services after US resettlement HHS public access. J Immigr Minor Heal. 16(5):1016–22
Painter RC, Roseboom TJ, Bleker OP. 2005. Prenatal exposure to the Dutch famine and disease in later life: An overview. Reprod. Toxicol. 20(3):345–52
Stanner SA, Bulmer K, Andrès C, Lantseva OE, Borodina V, et al. 1997. Does malnutrition in utero determine diabetes and coronary heart disease in adulthood? Results from the Leningrad siege study, a cross sectional study. BMJ. 315(7119):1342–48
Tanner, James M. 1986. Growth as a mirror for the conditions of society: secular trends and class distinctions. In Human Growth: A Multidisciplinary Review. Arto Demirjian and Micheline Brault Dubuc, eds. Pp. 3-34. London: Taylor and Francis.
WHO. 2000. The Management of Nutrition in Major Emergencies. Link
